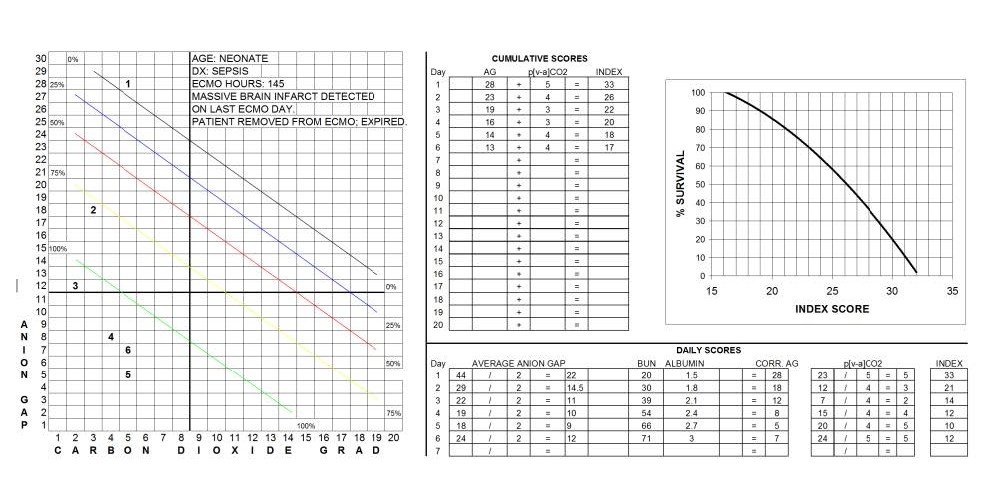
Example 3 Viability Index Score sheet illustrating a Day 1 VIS elevation beyond the point of no return with sluggish return to normal over a 72 hour period. The patient expired due to brain damage.
In Example 3, the Day1 Daily VI score of 33 plots at the very bottom of the survival curve. The Day 2 Daily VI score improves to only 21, demonstrating relatively sluggish recovery before the day 3,4,5 & 6 daily VI scores fall into an acceptable range. Even though the CVIS eventually falls to 17, the first VI score of 33 on the first ECMO day represents a ‘VI point of no return’ beyond which most patients will not survive. The ‘VI point of no return’ seems to be 32 or greater for all patients and probably quantifies the degree of intracellular acidosis resulting in irreversible damage to one or more vital organ systems.
There is probably a temporal component to the point of no return as well. Patients with a high VI for only a few minutes before extracorporeal support will probably have a better chance for survival compared to patients whose vital signs are supported with maximum medical management for hours or days but whose high VI fails to improve. The false reassurance of acceptable vital signs concomitant with a high VI can fatally delay the initiation of extracorporeal support.
The initiation of ECMO was too late to save the patient in Example 3 although the cause of death (a brain infarct) was not readily apparent until 5 days later. Monitoring of the VI before ECMO might have prompted earlier ECMO intervention at a lower VI and a better chance for survival.
Perfusion Theory is an educational platform for the Oxygen Pressure Field Theory (OPFT). August Krogh’s theoretical concept of the oxygen pressure field is explained and then applied to clinical applications in perfusion practice.