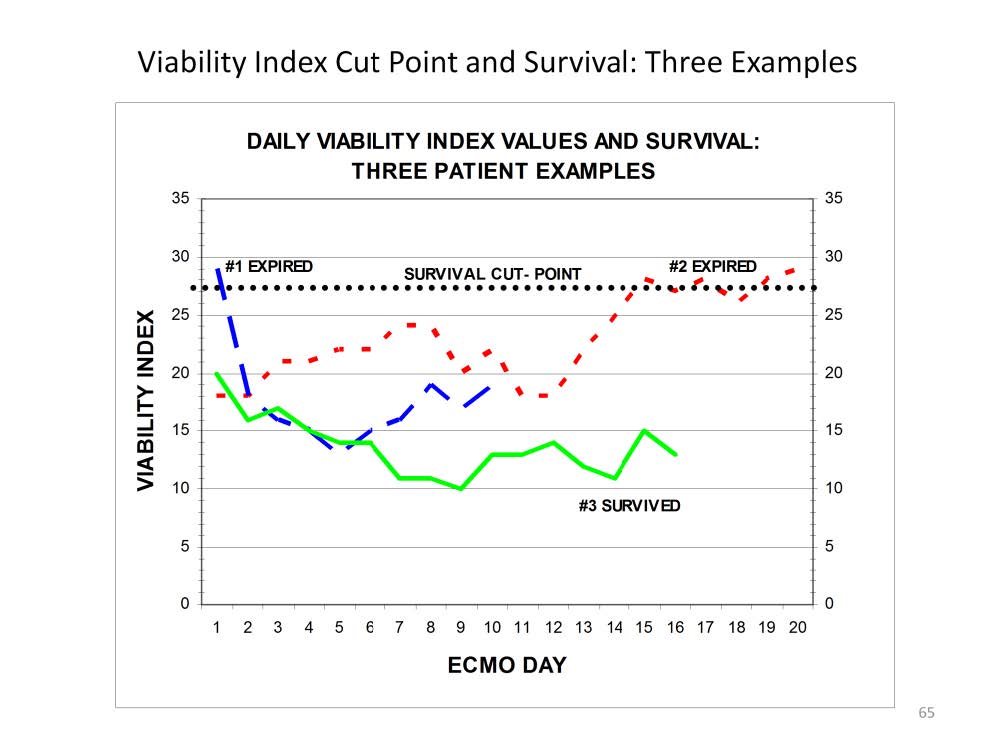
By systematically assessing the Viability Index (VI) over a period of time, the effectiveness of interventional support can be determined by the direction that the VI moves within the indeterminate area of the VI survival curve. For example, if the first VI on day 1 of ECMO is 24 but falls to 20 by the second day, this indicates that the intervention is effective. On the other hand, if the VI increases from 24 to 28, the intervention is not working and the patient will probably expire without a change in strategy. If a patient is placed on ECMO and develops a VI that exceeds the survival cut point, a fatal reperfusion injury may ensue even if prior or subsequent VI values are within a survivable range. In this figure are three examples of the daily Viability Index and survival.
Patient #1 (long dash line) had a moderate survival diagnosis (pulmonary hypertension: expected survival = 75%), but the VI on the first ECMO day exceeded the hypothetical survival cut point (dotted line). The remaining days on ECMO were all below the cut point. Patient died of a large brain infarct that was detected by head ultrasound on ECMO Day 10. This complication probably occurred on the first day as a result of reperfusion injury. Even though subsequent VI scores were in the normal range, the brain damage caused by reperfusion injury on the first day resulted in the patient’s demise.
Patient #2 (short dash line) had a low survival diagnosis (Pertussis: expected survival = 30%). The VI remained below the survival cut point for the first 14 ECMO days, but then rose above the cut point during the final week on ECMO. Patient died of multi-system organ failure, the pulmonary disease never having improved.
Patient #3 (solid line) had a moderate survival diagnosis (sepsis: expected survival = 75%). The VI during ECMO never exceeded the hypothetical survival cut point, so the patient was not at risk for lethal reperfusion injury. Patient survived without complications.
Perfusion Theory is an educational platform for the Oxygen Pressure Field Theory (OPFT). August Krogh’s theoretical concept of the oxygen pressure field is explained and then applied to clinical applications in perfusion practice.