The survival of ECMO patients is correlated to the average AGc and the average p[v-a]CO2 during the ECMO run. A related method looks at the very first AGc and p[v-a]CO2 just before or just after the beginning of ECMO. At the micro-vascular tissue level, the AGc detects tissue anoxia and the p[v-a]CO2 detects tissue carbon dioxide retention, both of which are caused by poor perfused capillary density. Together, these risk markers detect tissues with localized hypoxic ischemia which is caused by various types and degrees of shock.
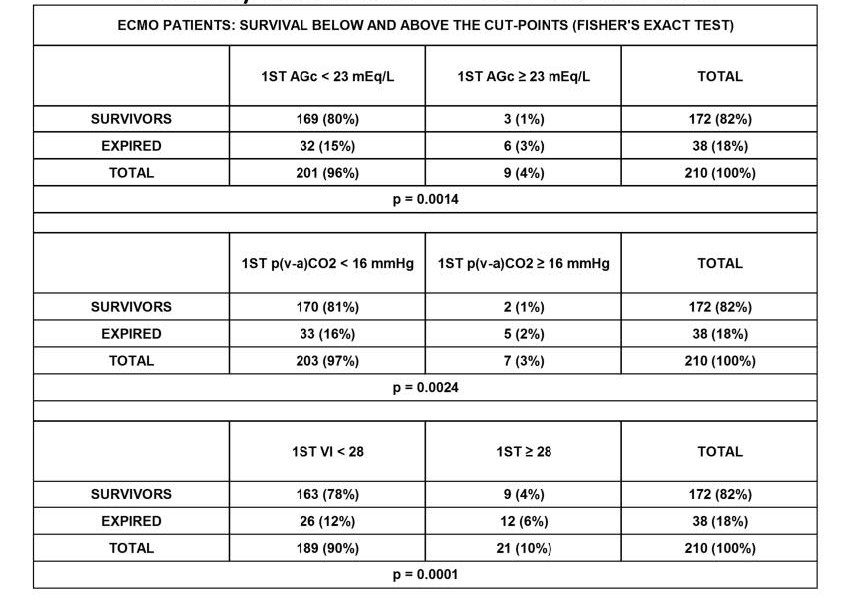
The first AGc beyond 22 mEq/L or the first p[v-a]CO2 beyond 15 mmHg (both of these are cut points) predict certain patients as being high risk as illustrated in the table above. Unfortunately the first AGc by itself only identifies 9 (4%) of the 210 ECMO patients as high risk and the first p[v-a]CO2 by itself only identifies 7 (3%) of the 210 ECMO patients as high risk. Generally any AGc elevated above the highest normal value (>14 mEq/L) usually indicates that the tissues are experiencing some degree of hypoxia. Any p[v-a]CO2 above the highest normal value (>7 mmHg) indicates that the tissues are experiencing some degree of carbon dioxide retention. Moderately elevated AGc values or moderately elevated p[v-a]CO2 values by themselves are not necessarily lethal. The cells can tolerate one or the other up to a certain cut point; < 16 mmHg for the p[v-a]CO2 and < 23 mEq/L for the AGc.
In contrast, the first Viability Index identifies 21 (10%) of the 210 ECMO patients as high risk, two to three times more than the first AGc alone or the first p[v-a]CO2 alone. If both the AGc and the p[v-a]CO2 are moderately elevated at the same time (even to levels less than the cut points), cells are less capable of tolerating the dual effects of hypoxia and carbon dioxide retention simultaneously. These effects are apparently cumulative which explains the need to monitor the Viability Index. The Viability Index measures the extent of this dual effect; reaching its lethal tipping point at 28.
Perfusion Theory is an educational platform for the Oxygen Pressure Field Theory (OPFT). August Krogh’s theoretical concept of the oxygen pressure field is explained and then applied to clinical applications in perfusion practice.