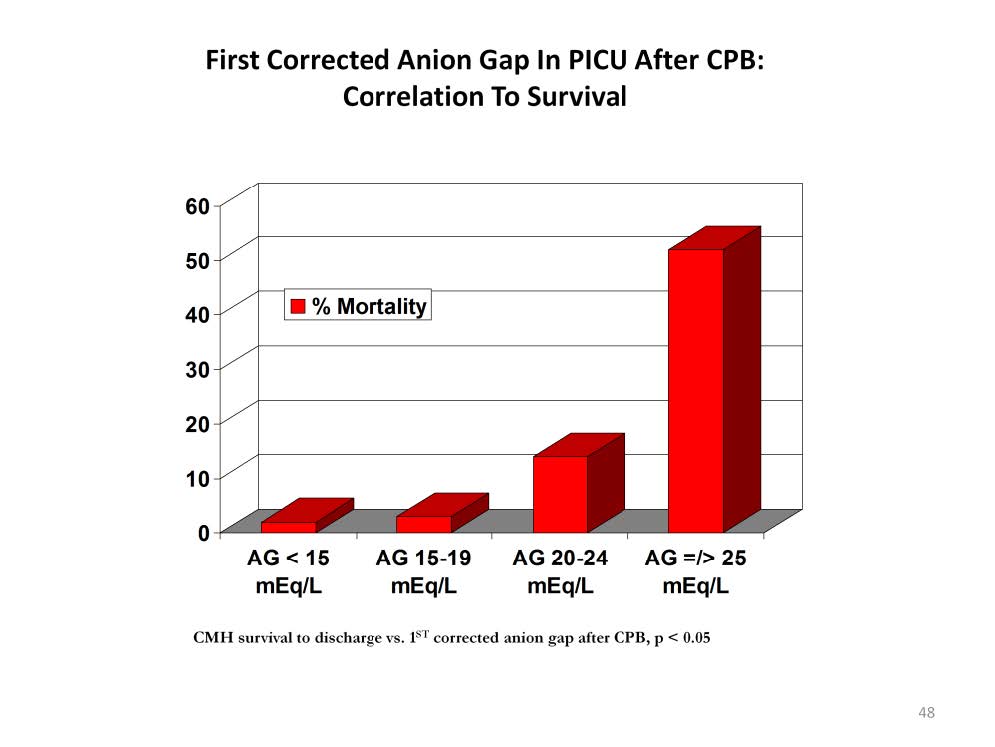
In the post operative period after congenital heart surgery, the initial AGc is indicative of how well the patient tolerated the surgery. Subsequent measurements indicate if the patient is improving or worsening. This chart illustrates the predictive capacity of the 1st corrected anion gap (AGc) measured in the ICU after congenital heart surgery. The higher the post operative AGc the greater the mortality. Patients with a normal AGc (< 15 mEq/L) have less than 1% mortality and those with a AGc of 25 mEq/L or higher have a mortality greater than 50%.
The AGc quantifies tissue hypoxia independently of other physiologic and hemodynamic assessments. Lactates used to assess the adequacy of tissue oxygenation often peak several hours after the maximum AGc. Waiting for lactate levels to reach the *LD50 can delay the implementation of effective extracorporeal intervention.
* The lethal dose level at which 50% of the patients die. For lactate the value is about 11 mmol/L. If the normal range for the anion gap is 7-14 mEq/L, a lactate of 11 mmol/L would increase the anion gap to 18-25 mEq/L.
Perfusion Theory is an educational platform for the Oxygen Pressure Field Theory (OPFT). August Krogh’s theoretical concept of the oxygen pressure field is explained and then applied to clinical applications in perfusion practice.