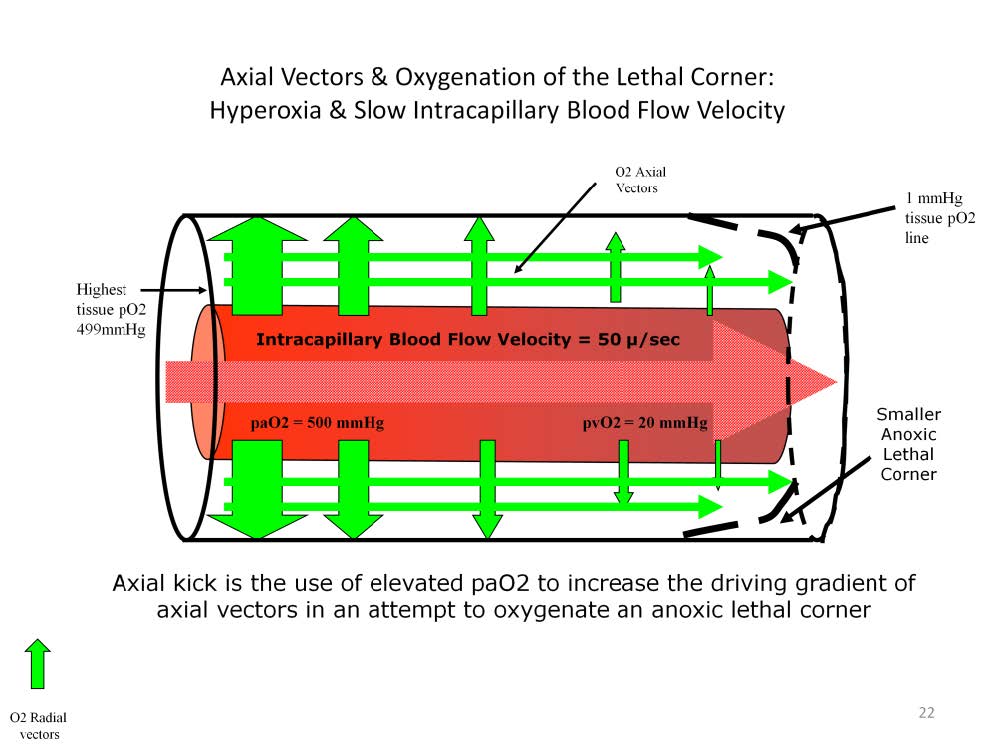
Hyperoxia does not significantly increase the oxygen content of arterial blood, but it does help to redistribute oxygen to lethal corner areas along axial vectors during period of low blood flow or poor PCD.
The perfusionist who understands this axial vector phenomenon can compensate somewhat for pathologic or iatrogenic low flow states by increasing the pO2 of the arterial blood. For example, increasing the arterial pO2 from 80 to 500 mmHg floods the arterial-end tissues with oxygen and increases the axial gradient. This increased axial gradient then results in axial vectors that can extend into the lethal corner area, helping to suppress the formation of an anoxic lethal corner until blood flow can be restored. For example, during cardiopulmonary bypass or ECMO the blood flow may be lowered temporarily to facilitate a certain surgical or medical procedure. During this time period the patient may benefit from having the oxygenator sweep gas FiO2 increased to 100% to augment axial oxygen vectors. However this is only a temporary solution to a low blood flow condition. As discussed previously, if intracapillary velocity or PCD is decreased for too long a hypercapnic lethal corner can result.
Perfusion Theory is an educational platform for the Oxygen Pressure Field Theory (OPFT). August Krogh’s theoretical concept of the oxygen pressure field is explained and then applied to clinical applications in perfusion practice.