The carbon dioxide pressure field normally has small gradients due to the high solubility of CO2. The formula for calculating the cardiac index using the venoarterial CO2 gradient comes from Johnson & Weil, 1991.
The formation of an anoxic lethal corner is not the only mechanism that can result in tissue acidosis. The trapping and retention of carbon dioxide in the lethal corner area also occurs and can be described using the Krogh cylinder model. This phenomenon is particularly deadly because it is almost totally unknown to clinicians caring for critically ill cardiopulmonary patients and it can occur without any deviation of the arterial blood gas from normal values or a change in hemodynamic parameters.
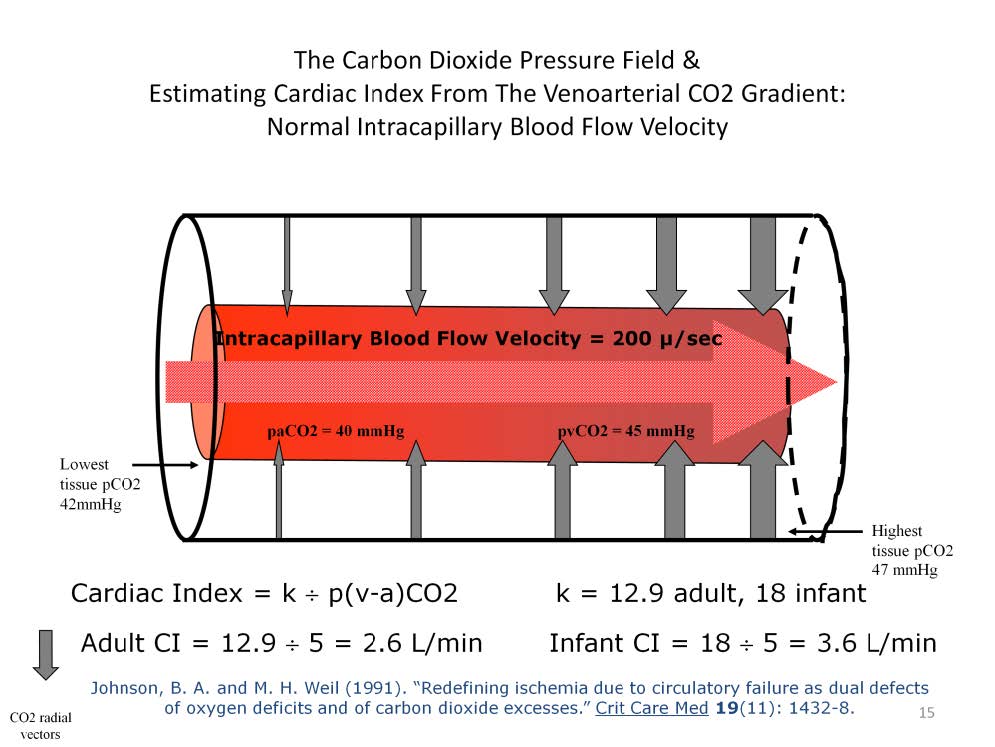
There is a carbon dioxide pressure field but it does not normally have the large range of values like those seen in the oxygen pressure field . Carbon dioxide is 23 times more soluble in water than oxygen, so it requires only 1/23rd the gradient needed by oxygen for removal from the Krogh cylinder. Carbon dioxide has its highest concentration in the distal corner of the Krogh cylinder and its lowest concentration at the capillary’s proximal end, nearest the capillary wall; the opposite configuration of the oxygen pressure field. In this illustration, the arterial blood pCO2 is 40 mmHg and the arterial-end tissue pCO2 is 42 mmHg. The venous blood pCO2 is 45 mmHg and the venous-end tissue pCO2 is 47 mmHg. As long as the intracapillary velocity of the blood remains normal (~200μ/sec) and the diameter of the Krogh cylinder does not change, then adequate amounts of carbon dioxide will be removed from the tissues. The evidence of this is a normal venoarterial carbon dioxide gradient (p[v-a]CO2) which is about 5 to 7 mmHg. Since the p[v-a]CO2 is in part dependent on the intracapillary velocity of the blood, the cardiac index can be estimated from the p[v-a]CO2. In adults, dividing the constant “12.9” by the p[v-a]CO2 gives an estimate of the cardiac index with R=0.76 and R2 = 0.58. In the younger the patient, the constant is larger. This is because of the higher metabolic rate in younger patients. In infants the constant is estimated at 18.
Perfusion Theory is an educational platform for the Oxygen Pressure Field Theory (OPFT). August Krogh’s theoretical concept of the oxygen pressure field is explained and then applied to clinical applications in perfusion practice.