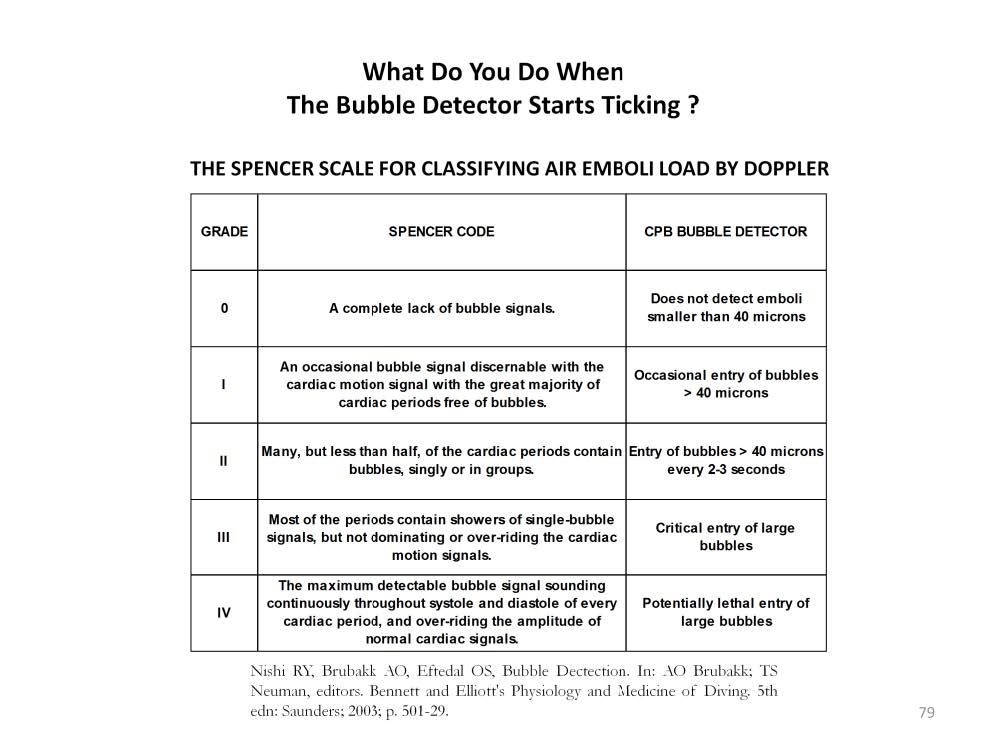
The Spencer scale was developed by Dr. Merrill P. Spencer MD, PhD (1922-2006) in the 1960’s using Doppler devices over the hearts of divers. This scale is quite subjective, but basically, if no bubbles are heard that equals Grade 0. Grade I has a few bubbles. Grade II has more bubbles. Grade III is many bubbles. And lastly, Grade IV has continuous bubbles throughout the cardiac cycle. During the process of decompression, this scale is useful for determining the presence and quantity of bubbles in the divers’ blood stream. The decompression process is slowed down if the frequency and quantity of bubbles is too high.
The risk of bubbles passing through the circulation as measured by a Doppler can be classified according to the Spencer scale. The risk increases as the frequency and quantity of bubbles increases. However there is no time frame on the Spencer scale. For example, a Class IV risk for a short time (minutes or seconds) might be enough to cause serious injury or death. But what about a Class I that lasts for two hours? Is the risk cumulative over time? In other words, which is more likely to cause damage in a CPB patient; lots of GME in a short time or a few GME over a long period culminating in a large volume having entered the patient. And once GME composed mostly of nitrogen have entered the patient, how can they be removed?
Perfusion Theory is an educational platform for the Oxygen Pressure Field Theory (OPFT). August Krogh’s theoretical concept of the oxygen pressure field is explained and then applied to clinical applications in perfusion practice.