High perfused capillary density (PCD) and oxygen loading can reduce the development of acidosis during the period of hypothermia arrest. There are four discrete gas strategies that perfusionists can employ to prepare the patient for deep hypothermia circulatory arrest (DHCA); 2 for carbon dioxide and 2 for oxygen:
Pearl JM, Thomas DW, Grist G, Duffy JY, Manning PB. Hyperoxia for management of acid-base status during deep hypothermia with circulatory arrest. Ann Thorac Surg 2000;70:751-5.
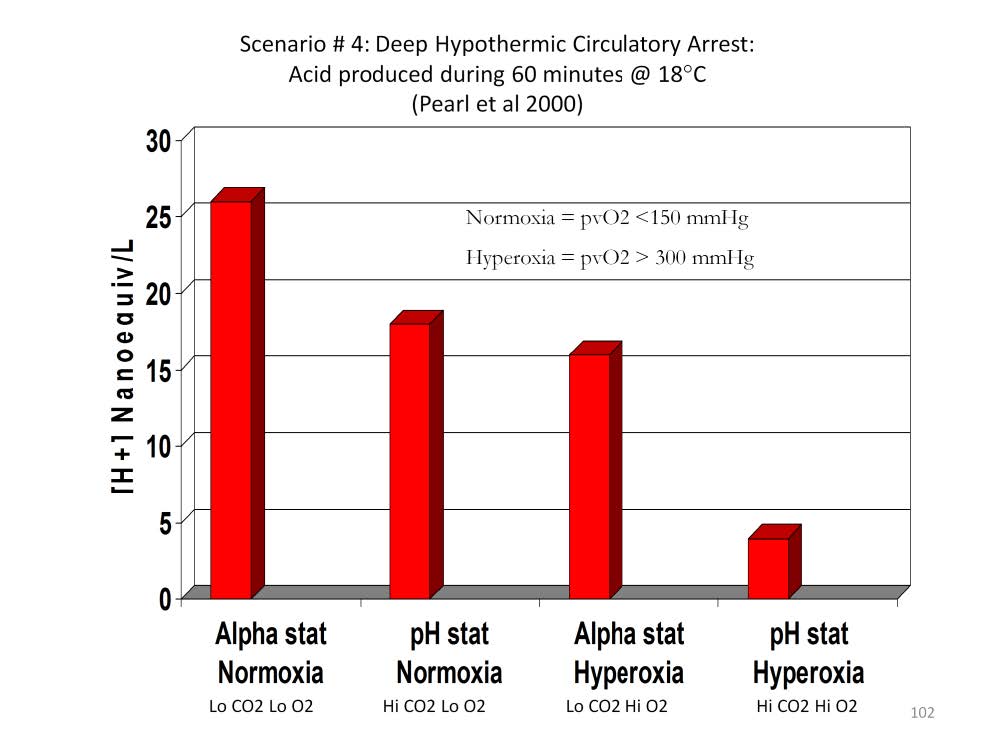
BACKGROUND: Which blood gas strategy to use during deep hypothermic circulatory arrest has not been resolved because of conflicting data regarding the advantage of pH-stat versus alpha-stat. Oxygen pressure field theory suggests that hyperoxia just before deep hypothermic circulatory arrest takes advantage of increased oxygen solubility and reduced oxygen consumption to load tissues with excess oxygen. The objective of this study was to determine whether prevention of tissue hypoxia with this strategy could attenuate ischemic and reperfusion injury.
METHODS: Infants who had deep hypothermic circulatory arrest (n = 37) were compared retrospectively. Treatments were alpha-stat and normoxia (group I), alpha-stat and hyperoxia (group II), pH-stat and normoxia (group III), and pH-stat and hyperoxia (group IV).
RESULTS: Both hyperoxia groups had less acidosis after deep hypothermic circulatory arrest than normoxia groups. Group IV had less acid generation during circulatory arrest and less base excess after arrest than groups I, II, or III (p < 0.05). Group IV produced only 25% as much acid during deep hypothermic circulatory arrest as the next closest group (group II).
CONCLUSIONS: Hyperoxia before deep hypothermic circulatory arrest with alpha-stat or pH-stat strategy demonstrated advantages over normoxia. Furthermore, pH-stat strategy using hyperoxia provided superior venous blood gas values over any of the other groups after circulatory arrest.
Perfusion Theory is an educational platform for the Oxygen Pressure Field Theory (OPFT). August Krogh’s theoretical concept of the oxygen pressure field is explained and then applied to clinical applications in perfusion practice.