Pathologic or iatrogenic decreases in PCD can result in exponential increases in CO2 retention within the lethal corner area.
A decrease in intracapillary blood flow velocity is, theoretically, an important cause of the linear retention of carbon dioxide in the lethal corner. However the result of a decreased cardiac index would more likely result in a reduction of PCD. An exponential increase rather than a linear increase in the retention of carbon dioxide would then occur, resulting in a hypercapnic lethal corner.
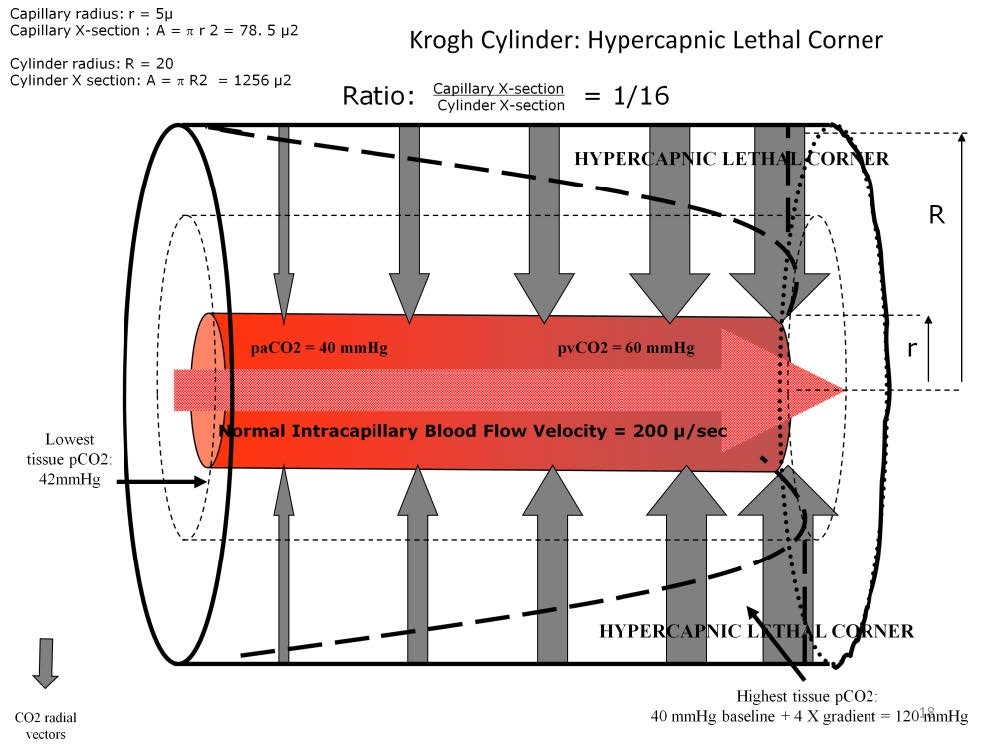
If PCD decreases and the cylinder radius doubles, the capillary-to-cylinder ratio changes from 1:4 to 1:16. Since the tissue volume around the open capillary has increased by almost a factor of four, this single capillary will need to remove four times more carbon dioxide than it normally would in a 1:4 cylinder. This will overload the capillary’s capacity to remove carbon dioxide from the tissues and cause the massive retention of carbon dioxide within the lethal corner. If the patient experiences both a reduction in intracapillary blood flow velocity and a decrease in perfused capillary density the retention of carbon dioxide in the lethal corner can be tremendous. An estimate of the carbon dioxide trapped in the lethal corner tissues can be made by adding the arterial pCO2 to four times the p[v-a]CO2. In this example, the lethal corner carbon dioxide concentration would be about 120 mmHg. Unless this situation is reversed quickly by increasing the blood flow and increasing perfused capillary density, the patient will expire.
A goal directed therapy that focuses on oxygen delivery may miss the development of a hypercapnic lethal corner because the arterial pCO2, arterial oxygen saturation and even the hemodynamics may be normal. But at some point the patient’s organ function will begin to falter due to the hypercapnic lethal corner.
Perfusion Theory is an educational platform for the Oxygen Pressure Field Theory (OPFT). August Krogh’s theoretical concept of the oxygen pressure field is explained and then applied to clinical applications in perfusion practice.