Reductions in PCD can result in exponentially large increases in the Krogh cylinder configuration leading to the development of a lethal corner.
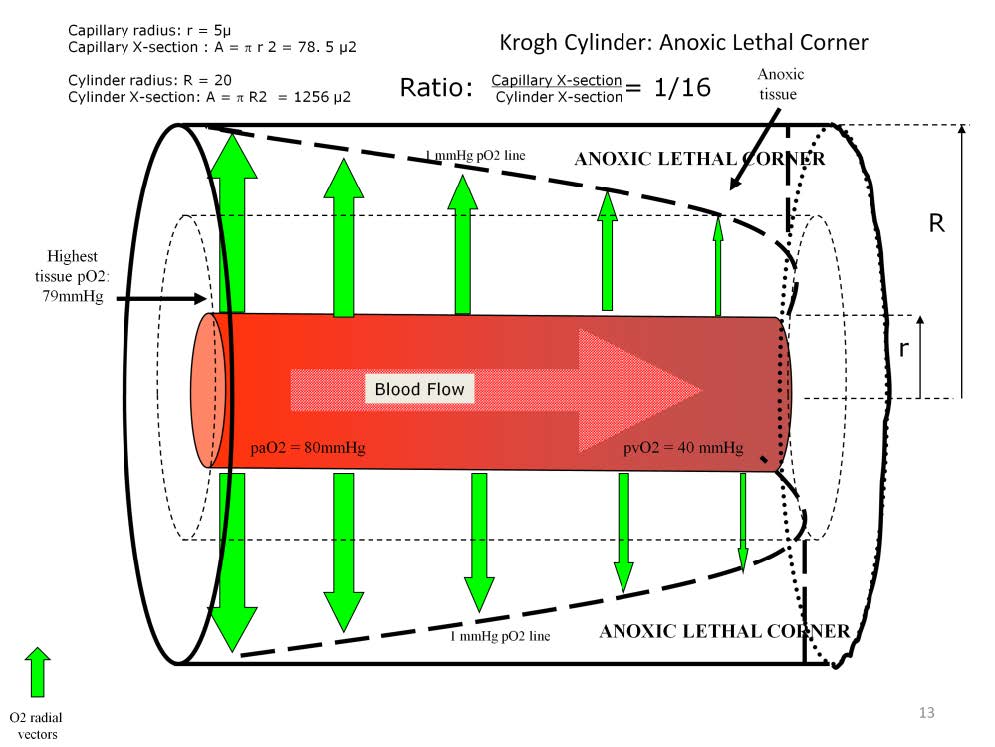
During a disease state, cardiac output may not be able to increase or even maintain the volume necessary to preserve adequate homeostasis. PCD becomes less than is required to meet the demands of the tissues. So the Krogh cylinder becomes too large and too deep to allow for the adequate distribution of oxygen to the needy mitochondria and removal of acidifying carbon dioxide. Reduced PCD changes the relationship between the capillary cross-section and the cylinder cross-section. The Krogh cylinder seen here develops as a result of a pathologic or iatrogenic reduction in PCD. The capillary radius is still 5μ, but the cylinder radius has increased from 10 as seen in the previous model to 20μ, making the capillary-to-cylinder cross-sectional ratio 1:16. This cylinder is too large for the radial vectors to adequately oxygenate the tissues surrounding the distal capillary. This capillary then fails to provide enough oxygen to a tissue volume that is almost 4 times greater than seen in the earlier 1:4 cylinder example. The result is an area of anoxic tissue called the ‘lethal corner’ near the distal periphery of the cylinder.
The oxygen pressure field within this cylinder has a range of 79 mmHg to 0 mmHg, but the median value is only about 5 mmHg instead of 20 mmHg. So 50% of the tissues have pO2 values greater than 5 mmHg and 50% have values less than 5 mmHg with a large portion receiving no oxygen at all.
Even in a disease state, cardiac output may seem adequate, intracapillary blood flow velocity may seem normal and oxygen extraction may also seem normal. But radial vectors may be too low in magnitude to adequately fill the distal corners of a large cylinder with oxygen. So an anoxic lethal corner forms. The result is a situation where normoxic, hypoxic and anoxic mitochondria exist simultaneously within the same capillary bed. The size of the lethal corner is determined by the number of anoxic mitochondria present. Organic acid waste products accumulate in the lethal corner as the anoxic mitochondria convert to anaerobic metabolism. The tissue pH decreases impairing enzymatic function in local tissues and, ultimately, organ function as a whole. A common medical term used to describe this situation is “shock”.
The formation of an anoxic lethal corner may be an unrecognized but common complication of routine cardiopulmonary bypass. Despite the maintenance of vital perfusion parameters within the normal range a base deficit frequently develops on pump or in the immediate post-pump time period. This probably indicates a detrimental change in PCD during cardiopulmonary bypass.
Perfusion Theory is an educational platform for the Oxygen Pressure Field Theory (OPFT). August Krogh’s theoretical concept of the oxygen pressure field is explained and then applied to clinical applications in perfusion practice.