Part XVIII- Episode 1 – Buying Time- The Advent of Myocardial Protection – Standing on Tall Shoulders- The History of Cardiac Surgery Thomas N Muziani PA-C, CP
To give pleasure to a single heart by a single act is better than a thousand heads bowing in prayer”
-Mahatma Gandhi
Prologue-
I have received several requests for a more comprehensive backstory on myocardial protection. From my earliest days in medicine I have had a profound fascination with protecting the heart. Several years ago, during an eleven hour extracorporeal bypass, seven hour cross-clamp, I discovered nirvana. But I digress.
In 1968, as a direct result from a universal moratorium against utilizing potassium based cardioplegia, there remained two options for “stilling” a beating heart and avoiding air embolus; the copious application of cold solution or saline slush or the intermittent cross clamp with an electric fibrillator. The fibrillator at the time was basically two wires and capacitor with a switch plugged into alternating current…Nicola Tesla would have been proud. The ironic dichotomy is not lost; electricity can give life or take it away. Electrical shock to defibrillate for life…but add a chair, increase the alternating current…and quiet a heart and a life forever. We are a strange species.
It should be noted that at the time, virtually no research on any experimental model had been conducted as to myocellular repercussions applying an electrical current directly on the heart. The rationality was borderline medieval. A general assumption within the medical community for the better part of sixty years has been that ventricular fibrillation will trigger an elevation of serum troponin T levels. Elevated troponin T levels are a specific marker of myocardial injury and an independent predictor of early death in pediatric cardiac surgery patients. The causation for elevated troponin T has now been discovered to be direct electrical current applied to the heart, not ventricular fibrillation. In Germany, an exhaustive study at seven institutions on the effects of implantable auto-triggering pacemakers/defibrillator isolated the causation of elevated serum troponin T.
Cardiac myocytes are highly specialized extremely sensitive cells. In a recent (2017) conference of stem cell researchers, the general consensus agreed upon the complex matrix that forms a cardiac myocyte makes it extremely difficult to reproduce. Stimulating a cardiac myocyte either with direct electrical current or electro-mechanical infusion of potassium-ion is strange at best and very unkind to the sensitive fragile nature of the cardiac myocyte at minimum. No other animal in nature utilizes potassium to regulate their furnace.
If we convened a philosophical conclave with philosophers, mystics and clerics to discourse about the miraculous nature of the human heart…it would start with the observation that God, Yahweh or whomever plus the laws dictating natural selection intentionally enshrouded the heart and lungs in a protective cage, difficult to reach, because it is the sanctum sanctorum of the human body. Every other vital organ in a human is essentially fully exposed. This did not escape the Egyptians, Babylonians, Mayans, Aztecs and Incas. Heart enucleation was a sacred act.
Several surgeons passed along anecdotes about the horrors associated with early days of potassium arrest. This led to speculating as to why anyone would ever voluntarily choose potassium, of all mechanisms, to freely inject into a living heart with the sole intent on having that same heart return vibrant, beating and ejecting with force?
Sixty plus years later…it will still elicit animated arguments and extreme prejudice of technique.
The building blocks for myocardial preservation-
Sixty-three years have passed since the inception of modern open-heart surgery. The advent and utility of the new heart-lung machine opened the flood gates for creativity. For the very first time in human history plunging below the sternum to facilitate a corrective repair, close a congenital defect or stop unabated bleeding would not be fraught with severe time constraints, risk of air embolus or potential peril.
Despite the general assumption at the time that postoperative low-cardiac output syndrome was related to inadequate anatomical repair rather than the most likely cause of insubstantial myocardial protection…many outcomes were still viewed as “acceptable.” Patient leaving hospital was viewed as acceptable. The development of cardioplegic techniques has without question provided a more stable platform to facilitate lowering mortality rates in cardiovascular surgery. Today, the utilization of potassium-based electro-mechanical arrest is still the primary method of myocardial protection. The backdrop for the evolution of potassium-based cardioplegia, including the pariah atmosphere of the medical community during the 1960’s needs revisiting.
With any new journey, there are requisite first steps. Those first steps can be traced to an English physician and pharmacologist, Sidney Ringer. His laboratory was located in the old and rather poor section of London. While at University College London 1883 he published a seminal paper in the Journal of Physiology that described the antagonistic effects of calcium and potassium on cardiac contraction. How he arrived at this conclusion was pure serendipity…and truthfully, had very little to do with Sidney Ringer.
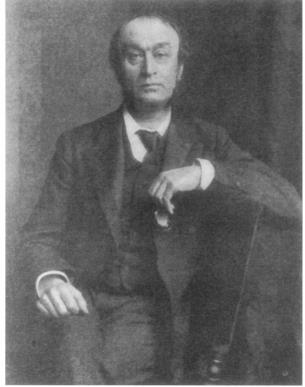
Dr. Sidney Ringer
Dr. Ringer had two very resourceful lab assistants that, by all accounts, performed the majority of preparation and figurative heavy lifting for their myriad experiments. They had prepared several frog hearts for totally unrelated study when they realized their water distillery had malfunctioned. In order to not upset the good doctor with failed experiments, they proceeded utilizing the well water from old London’s water system which, in some areas, dated to the 13th century. To their amazement, the frog hearts “ceased activity” almost immediately when injected with well water. When they repeated the experiment with their distilled water, the frog hearts maintained a syncopated forceful rhythm.
Ringer reported that if calcium was left unopposed by potassium salts, contractions strengthened until fusion of beats occurred and ventricular tetani ultimately resulted. Conversely, incremental increases of potassium resulted in weaker and weaker beats until cardiac asystole developed. Subsequent work by a multitude of physiologists in the late 19th and early 20th centuries extended Ringer’s findings and therefore provided the basis for the ionic theory of cardiac activity.
Over fifty years elapsed after Ringer’s paper when D.R. Hooker utilized potassium-induced elective cardiac arrest to revive victims subjected to inadvertent electrical shock. The corrective dogma at the time for treating ventricular fibrillation was to stop the “bag of worms” before allowing it to beat again. Then, in 1929, Hooker wrote about the experimental use of potassium chloride to resuscitate dog hearts subjected to ventricular fibrillation; upon coronary infusion of potassium chloride the canine hearts stopped; and after washout of the potassium solution, a coordinated ventricular rhythm resumed. The concept of utilizing potassium as an agent for arrest would have to wait another 20 years until Henry Swan would revive this work to combat ventricular fibrillation in severe hypothermic patients.
Although it was generally acknowledged that sodium, calcium and potassium maintained a very intimate relationship with cardiac activity no one seemed to be willing to describe each ion’s individual effects. Finally, in 1931, A.M. Baetjer and C.H. McDonald provided the first comprehensive description of the three ions. According to their papers, they detailed how sodium was chiefly responsible for the instigation and maintenance of spontaneous rhythmic contractions of the heart. Calcium asserted an essential element for the production of strong, mechanical contractions. Potassium displayed a profound antagonistic effect on calcium and, from all appearances, seemed to regulate an interaction between calcium and sodium.
C.R. Spealman observed that most investigators prior to 1940 used completely different compositions of the ionic concentrations from the standard Ringer’s solution. He set out to determine the effects of augmenting the concentrations of sodium, calcium and potassium within “physiologically normal” limits. An increase in calcium-ion concentration augmented both the amplitude and duration of the ventricular response. Increasing the potassium-ion concentration displayed a decrease in both atrioventricular (a-v) time interval and duration of ventricular systole. There appeared to be no discernable effect when sodium-ion concentrations were augmented within “normal” range.
As has been mentioned in previous articles, there seems to have developed a “dark age” during the early 20th century regarding cardiac corrections. The preponderance of evidence for this seems to emanate from the prejudicial bias of peers regarding either the profound belief that hearts could not be repaired or should not be repaired. Venturing into this very public arena with either a publication or providing a lecture could produce a response very similar to being thrown into Vespasian’s Colosseum in Rome during the bloody public games era with “Lions three, Christian’s zero” types of outcomes. Pity the poor soul that surmised a repair for the treatment of mitral valve disease, an open atrium or ventricular septum.
Therefore, the future of clinical cardiac repair seemed dismal in the 1920’s. However, the military surgeons forged ahead with breakthrough surgeries during the early 20’s, 30’s and 40’s when everyone else feared to tread. A totally new breed of cardiac surgeon emerged in the 1930’s and 1940’s. History has corroborated throughout the millennia, the advancement of surgery, especially cardiac, has a direct proportional relationship with the empirical knowledge gleaned from combat. War provides the surgeon several advantages and “test subjects” that lay physicians unfortunately will never have access to;
- You are working on an otherwise very healthy, well conditioned individual
- Your decision making process is, more often than not, a true emergency based upon saving a life. Therefore, any corrective action must be considered a positive action. Combat surgeons triaged patients and they always treated…even if it was only to hear last wishes.
- Because this is the military, potential litigation becomes a non-issue, therefore non-impediment.
One shining example was Dr. Elliot Cutler. Returning to Peter Bent Brigham in Boston, MA after his tour as a combat surgeon during World War I, he boldly ventured into the lions pit. Realizing a little 12 year old girl was dying from rheumatic mitral stenosis, he performed the world’s first closed transventricular mitral commissurotomy with a tenotomy knife.
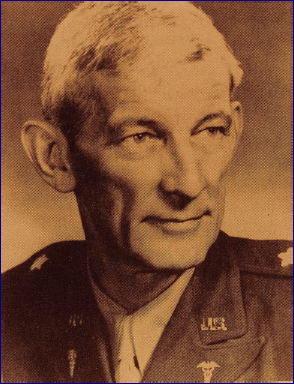
Brigadier General Dr. Elliott Cutler
These veterans did not suffer fools lightly, nor were they tolerant of voodoo medical doctrine. The post war surgeons forged ahead in the development of operative techniques for the treatment of congenital anomalies. By the mid to late 1940’s surgeons were willing to attempt a repair on atrial septal defects. However, out of necessity, all of these procedures were considered “closed”, therefore the results were all too commonly considered suboptimal. The heart-lung machines available at the time were rare and usually only at large, financially well-endowed hospitals.
They were cumbersome and considered unsafe if cavalier in its utility. While perusing the history books, it became obvious that the fault had nothing to do with the mechanical limitation of the heart-lung machine itself…but the oxygenator. These heart-lung machines during this period were designed and assembled at their respective institutions. Mayo Clinic had a design. Stanford had a design. Oxygenators varied as well. The more complicated the machinery, the more individuals required to operate it. Open cardiac repairs that facilitated unhurried, direct-vision corrections working on an empty heart were mandatory if clinical results were to improve.

Mayo Clinic Heart Lung Machine

Mayo Clinic Heart Lung Machine