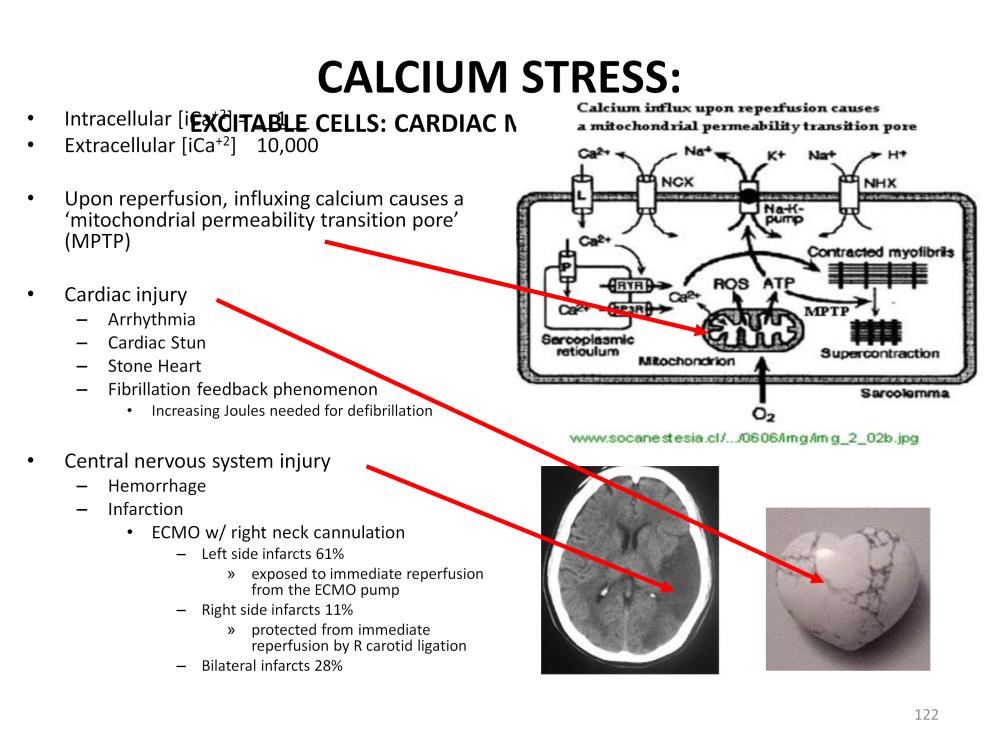
The second major mechanism of reperfusion injury is calcium stress. This is also called a paradox because living systems need calcium for normal cellular processes. But the uncontrolled influx of calcium into the cell or release of calcium from intracellular storage sites (such as the sarcoplasmic reticulum) after ischemia results in mitochondrial damage called a ‘mitochondrial permeability transition pore’ or MPTP*. This occurs in excitable cells such as cardiac conduction cells, cardiac myocytes and neurons.
The MPTP causes mitochondrial membrane swelling and the uncontrolled release of ATP from the mitochondria. In cardiac myocytes, this causes normally contacting myofibrils to super contact and not relax. Over time, as more and more myofibrils super contact, the heart becomes stiffer and less efficient at pumping. During CPR resuscitation the efficiency of chest compressions is reduced as the heart stiffens. More preload is needed and more robust compressions are required to maintain the same systemic perfusion. A fibrillation feedback condition also develops wherein increasing energy (Joules) is needed for defibrillation each time the heart fibrillates until a point is reached when the heart will not respond to defibrillation.
The reversible form of this cardiac myocyte hypercontracture is known as ‘cardiac stun’. Hypercontracture can progress to the point where the cardiac contracture/relaxation cycle is very poor and the heart muscle irreversibly damaged; a condition known as ‘stone heart’.
The MPTP effect can be particularly damaging to the central nervous system (CNS). In the typical ECMO patient with right neck venoarterial cannulation, the CNS damage by infarction occurs most often in the left brain. At first, this seems illogical because the right brain’s blood supply is greatly diminished by the ligation of the right carotid artery. However once the patient is placed on ECMO, the left carotid will immediately carry warm, well oxygenated blood directly to the left brain. If reperfusion injury potential is present in the brain, significant left sided CNS damage will occur. The right brain, although deprived of much of its circulation, is more or less protected from sudden reperfusion from the ECMO pump. Blood gradually enters the right brain from the right vertebral artery and circle of Willis after first passing through other parts of the body and mixing with non-ECMO blood. This reduces the oxygen and calcium levels before the blood enters the right brain. The incidence of left brain infarctions is almost 6 times greater than right brain infarctions, even though the right carotid is ligated prior to ECMO.
*Halestrap AP. Calcium, mitochondria and reperfusion injury: a pore way to die. Biochem Soc Trans 2006;34:232-7.
Perfusion Theory is an educational platform for the Oxygen Pressure Field Theory (OPFT). August Krogh’s theoretical concept of the oxygen pressure field is explained and then applied to clinical applications in perfusion practice.